








News and views
Stay informed with updates and expert insights on key developments shaping clinical practice.
Are humans the weakest link in clinical safety?
Oct 6, 2025, 10:00
by
User Not Found
Exploring AI oversight in medicine, questioning human‑in‑the‑loop models and how responsibility may shift as clinical artificial intelligence advances. Raj Rattan, Global Adviser, shares.
Following the launch of the AI Safer Practice Framework, Raj Rattan, Global Adviser at Medical Protection, reflects on what artificial intelligence means for clinical judgement, oversight and patient safety.
The AI Safer Practice Framework
The AI Safer Practice Framework is made up of two parts: INFORMED and RECORDS.
INFORMED guides ethical decision‑making using AI, while RECORDS documents AI‑assisted decisions for accountability and clinical rationale. The framework has been structured around these acronyms to ensure it is practical and memorable.
Learn more: AI Safer in Practice
Innovation in medicine and the rise of artificial intelligence
Advancements in medicine and dentistry have been driven by developments in materials science and technology. From the high‑speed handpiece to digital radiography and CAD/CAM, innovation has reshaped clinical practice – what we do and how we do it.
Artificial intelligence (AI) represents something different. It is an evolving system capable of interpreting data, analysing images, predicting outcomes, and sometimes recommending interventions. The future we imagine is already pressing at our door such is the pace of development.
AI oversight and the limits of human‑in‑the‑loop models
At the centre of today’s debate on AI in healthcare is the question of oversight. Most current frameworks, including our INFORMED framework, emphasise human‑in‑the‑loop (HITL) systems – AI outputs that are supervised, validated, and ultimately signed off by a human clinician. The logic is straightforward, humans bring professional judgement, context, and accountability. In this way, the dentist is seen as the strong link in the chain, ensuring that patient safety is not compromised by technology and algorithmic limitations. ¹
This assumption deserves closer examination. Why do we believe that humans always get it right? The medicolegal case experiences tell us otherwise. Clinicians are fallible. Diagnostic error remains one of the leading causes of harm in healthcare worldwide. Cognitive biases such as confirmation bias, anchoring, and availability heuristics distort decision‑making, even in experienced hands. Stress, fatigue, workload, and commercial pressures also take their toll. The truth is that the “human factor” is already a weak spot in clinical safety.²
By positioning HITL as the ultimate safeguard against AI error, we risk overestimating human reliability while underestimating human vulnerability. Take radiographic diagnosis for example, AI systems are already showing accuracy comparable to, and sometimes exceeding, that of dentists when detecting caries or periapical pathology.³
Defining the clinician’s role: the VIE model
What exactly is the healthcare professional’s role in overseeing these technologies? Let’s consider this under what I call the VIE model – see Figure 1 – which offers a way of framing this responsibility. It is a continuum of development in dental oversight: beginning with verification as the foundation, expanding through interpretation to add clinical meaning, and extending into enablement as AI becomes more autonomous. Each stage builds on the previous one, reflecting the profession’s evolving role in safeguarding safety, trust, and ethical practice as technology advances.
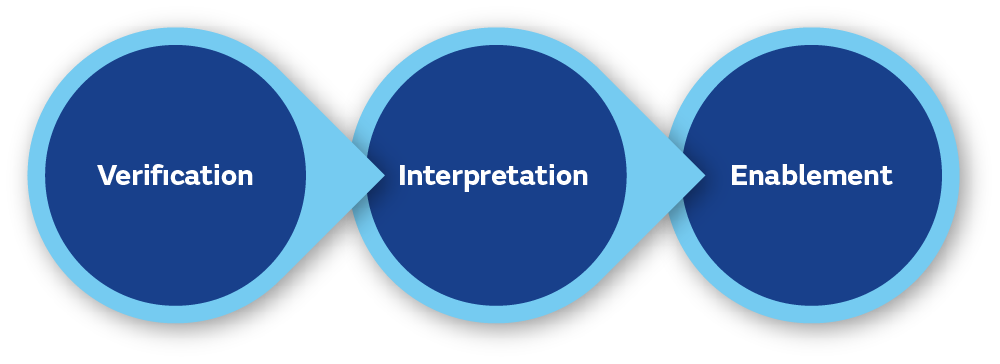
Figure 1: The VIE model. A shift from verification in the present to enablement in the future.
The paradox of progress
As AI continues to improve, the difference between human and machine performance may widen. The clinician may increasingly become the weak link, slower – although that may be an asset – more inconsistent, and more error‑prone than the technology. At that inflection point, the original logic of HITL starts to reverse. Instead of being the strong link that corrects machine error, the human risks becoming the weak link that introduces error into an otherwise reliable system. It is an unsettling paradox.
The current position on clinical responsibility
I must stress that I not suggesting the trust and reliance of human oversight is misplaced. Quite the opposite. At present, AI systems remain fragile, they lack transparency and are vulnerable to bias in their training data. AI cannot fully understand the human dimensions of care – patient values, preferences, and context. The clinician is still essential, not just for validating outputs but for discussions around uncertainty of outcomes and gaining consent for example. These responsibilities cannot be delegated to algorithms.
Looking ahead to autonomous AI in healthcare
We must also look ahead. Large language models (LLMs) and other generative AI systems are advancing rapidly. Their ability to synthesise information, adapt to context, and mimic reasoning suggests that autonomous AI in healthcare may be on the horizon.
When that day arrives, the key question will not be whether humans should stay in the loop, but whether the loop itself should be redesigned.
We cannot cling to the belief that human oversight will always be the gold standard of safety. Instead, we must be realistic about both the strengths and limitations of human judgement, and we must develop governance frameworks that can evolve as the balance of responsibility between humans and machines change.⁴
Facing the future with clarity
We must approach it neither with blind optimism nor paralysing fear, but with reason and clarity. LLMs may also lay the groundwork for a different future – one in which autonomy in AI is an operational reality.
As I finish editing this article, I take a short break and check my emails. There is an email from an AI developer with whom I have spoken before. The subject of the email reads ‘autonomous AI’ and attached to the email is a non‑disclosure agreement.
I am reminded of Einstein’s words: I never think of the future. It comes soon enough.
It just did.
About Medical Protection
Medical Protection exists to protect, support and advocate for doctors and health professionals throughout their careers. As the world’s leading member‑owned defence organisation, we combine decades of medicolegal expertise with practical support, education and professional indemnity designed around the realities of medical practice. By sharing insight drawn from real cases and investing in initiatives that support wellbeing from the very start of a career, we help reduce risk before it leads to complaints, claims or harm to patients. Our aim is not only to respond when things go wrong, but to provide the reassurance, knowledge and protection medical professionals need to practise with confidence.
References
1. Shortliffe, E. H. & Sepulveda, M. J. (2018). Clinical decision support in the era of artificial intelligence. JAMA, 320(21), 2199-2200.
2. Topol, E. J. (2019). Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again. Basic Books.
3. Rajpurkar, P., Chen, E., Banerjee, O. & Topol, E. J. (2022). AI in health and medicine. Nature Medicine, 28(1), 31-38.
4. European Commission (2024). Artificial Intelligence Act. Brussels.
Leave a comment