








Doing everything right after doing something wrong
10 Oct 2025
Estimated read time:
6 min read
Lucy Gibberd, Medicolegal Consultant at Medical Protection, shares a case where a doctor made an error but took immediate and appropriate actions in response.

Patient, Mr C, was in hospital for a planned musculoskeletal operation. He was seen in the pre-op area by a very experienced anaesthetist, Dr A, who discussed the planned anaesthetic and obtained informed consent. Dr A was planning a general anaesthetic for the duration of the surgery, with a regional anaesthetic block placed prior, that would provide postoperative pain relief. It was Dr A’s practice to place such regional blocks under ultrasound guidance while the patient was sedated but still awake. This allows monitoring by verbal feedback that the injection is proceeding as expected and is not unduly painful.
Dr A then returned to the empty theatre to draw up the medication that was required. In theatre the drug vials are found in the drawers of the anaesthetic trolley and as Dr A drew each drug into a syringe, he labelled each syringe with a self-adhesive, pre-printed, colour-coded drug sticker in accordance with international standards. He was not hurried or distracted and his working surface was uncluttered
Mr C was then transferred to the operating theatre where full monitoring was put in place, including blood pressure cuff, ECG and pulse oximetry. Dr A placed an intravenous cannula into Mr C’s right arm and then gave Mr C 3mls of an intravenous drug from a syringe that he had labelled as midazolam, a sedating agent. Dr A then turned away momentarily to pick up the equipment for the regional anaesthetic block. When he turned back and spoke to the patient, Dr A noticed he was not responding and appeared to be unable to move. Dr A immediately recognised, due to the close temporal relationship with a medication being provided, that there may have been a medication error and most likely a muscle relaxant, rocuronium, had been administered in error. The error was noted within less than a minute of the medication being administered and Dr A immediately alerted the anaesthetic technician to give him a breathing bag and airway to aid Mr C’s breathing and give supplemental oxygen. At the same time, he pushed the emergency bell and colleagues immediately appeared from the adjacent theatre to help. An anaesthetic colleague drew up propofol (an anaesthetic agent) and gave it to Mr C to induce anaesthesia (at approximately three minutes after the initial medication had been administered). This was the quickest way to relieve Mr C’s distress of being alert but unable to move. With the surgeon, a decision was made to continue with the planned surgery and an anaesthetic colleague took over for 15 minutes to allow Dr A to fill in an incident form immediately.
As soon as Mr C was awake after the surgery, Dr A explained what had happened openly and honestly and apologised for was undoubtedly a very distressing experience for Mr C. The error was also explained to Mr C’s wife around that time. The next morning Dr A phoned Mr C to again apologise, and the patient asked how this could have happened and how they were going to ensure it never happened again. Later that day, Dr A sent Mr C an email outlining what had happened. Dr A stayed in contact with the surgeon who saw Mr C for follow up in clinic and after a discussion with the surgeon, Dr A contacted Mr C again two weeks after the surgery.
On investigating the incident, Dr C noted that the hospital had recently changed suppliers for midazolam and the new vial (which was plastic) looked significantly different to the glass vial in which it had been supplied previously. Dr C had not been informed about the change and thinks that when he opened the drawer, he was looking for a glass vial. In addition, rocuronium is kept in a compartment immediately adjacent to the midazolam compartment in the drawer.
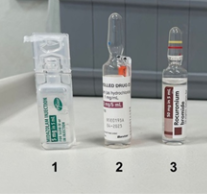
(1) The new midazolam plastic ampoule;
(2) the previous 5ml glass midazolam ampoule
(3) the 5ml glass rocuronium ampoule
Dr A noted that he always reads the ampoule as he draws up the drug and can only think that on that day his mind registered what he expected to see. He acknowledged that this was not an excuse and that he was responsible for checking the medication and he unreservedly apologised for the error that he made.
Mr C made a complaint to the Health and Disability Commissioner (HDC) noting that he sought compensation and a change in hospital procedures.
An ACC treatment injury claim was initiated by the operating surgeon to ensure that patient was covered by ACC for what had occurred. The hospital also offered to pay for counselling.
Medical Protection assisted Dr A in responding to the HDC complaint. Dr A acknowledged the error that he had made, took full responsibility for it and provided a sincere apology. He outlined the steps he had taken after the incident including filling in an incident form, openly disclosing the event to the patient as soon as that was possible, staying in contact with the patient afterwards and offering a meeting, being involved and open to self-reflection in a review of the incident and updating the processes in the hospital.
The hospital clinical governance team instituted a number of changes to ensure substitution errors would be less likely, including:
- That physically similar drug preparations, such as midazolam and rocuronium, should be stored apart.
- Pre-filled midazolam syringes could be offered as the standard preparation of midazolam.
- The anaesthetic trolley drawer partitions could be colour-coded to provide a strong visual reminder to those accessing the drawers of what type of drug they are reaching for.
- A designated pharmacist could be appointed to liaise with a designated anaesthetist regarding all decisions relating to drug purchasing and presentation of anaesthetic medications.
- A ‘purchasing for safety‘ drug policy could be developed that included avoiding purchasing look-alike packaging or labelling.
- Changes to the packaging or labelling of drugs should be widely communicated to all those involved in their storage and administration, including anaesthetists.
In many cases where a clinician has provided an incorrect medication which has harmed the patient, the clinician is found to be in breach of the Code of Rights. In this HDC decision, the Deputy Health and Disability Commissioner was critical that the error had occurred but considered the immediate actions that had been taken in response were appropriate, that there had been transparency and that changes had been actively considered and put in place to help prevent similar errors in the future. On that basis, Dr A was not found to have breached the patient’s Code of Rights, and no further action was taken against him.
Dr A agreed to allow us to describe what happened in this case with the intention of helping his colleagues become more aware of the possible dangers of substituting a medication and in the hope that that knowledge might help other clinicians avoid the error he made.
Learning points
- Clinicians are all human and can make errors, even when they are experienced and working in a non-emergency environment.
- When an error or an adverse event happens, clinicians will often be judged on their immediate actions and what they did afterwards to mitigate the harm and prevent similar issues in the future.
- The HDC expects that when an adverse event has happened, the patient will generally be informed ‘as soon as possible’ – as happened in this case.
- Continuing to follow up with a patient after an adverse event is an important part of providing good patient care.
- Being open in acknowledging the error and working to try to improve systems and their own practice, helps reassure both the patient and the regulator that the doctor is taking responsibility for what happened.
- Support from colleagues in the moment and aftermath, including a willingness to seek, acknowledge, and address latent system errors, can minimise harm and assist both the patient and doctor in finding some closure after an adverse event.


